The description says this video was uploaded only two months ago, but I could've sworn I saw this same video several years ago. Here's Vader versus Batman (and friends):
Wednesday, April 17, 2024
Tuesday, April 16, 2024
the Swiss are big mad and lead the way
Switzerland has had enough of the EU's nonsense.
Reminder: Switzerland is not an EU member.
mediquipped
 |
| pulse oximeter, CGM (constant glucose monitor), CGM manual |
 |
| CGM up close |
It was a disappointment to pick up the CGM, which seems a little backward and wonky. It requires initial calibration during its first two hours of use, then calibration every 12 hours after that. At the 15-day mark, you have to get another monitor to attach to your arm, and I guess the calibration has to happen again. I don't recall hearing about any of this with the monitors you get in the US, but maybe clever US marketing covered these troublesome details up. I'll read slowly through the user's manual and learn the machine's ins and outs.
As you see, I also got a pulse oximeter, so I can measure my pulse-ox. I doubt I'll use it often, but at those moments when I'm breathing harder than usual, it might come in handy.
One of the shop staffers spoke broken English, and he insisted on English the entire time. I tried to get him to switch to Korean, but then I thought that it might be better for him to keep speaking in English. While his English could definitely have used some help, he got his points across just fine. His English seemed only a little worse than my Korean.
threaten murder and see what happens
As Liberal Hivemind points out, it's always the liberals who threaten or enact violence, then turn around and claim it's the right that's constantly violent. Projection.
Hell, think about the recently deceased OJ Simpson. Were there conservative riots resulting in billions of dollars of property damage after the criminal-trial verdict? Ah, but how about the Rodney King case? Or the "summer of love"? Which stupid fuckers were rioting then?
What hypocrisy.
remember nutria/le ragondin?
Remember when I went to France in 2018, visiting my buddy Dominique at his bed-and-breakfast in le marais (the swamp/marshes), and learning from his son Tim about how there's a pest there called le ragondin, which Tim described in enough detail for me to realize he was talking about nutria, the same giant rat that lives in the Louisiana bayou? Well, here's a video about the nutria of the bayou, and how people hunt them to protect the ecology:
I'll always remember the pâté de ragondin I had in France. I was apprehensive at first, but who knew a rat could turn out to be so delicious? (It ended up tasting bland and like not much of anything. Still, not bad.)
"Dune, Part 2" will be mine!
My pre-ordered Apple TV copy of "Dune, Part 2" is coming today, so I hope to sit down and rewatch the movie tonight. Woo-hoo!
Iran attacks Israel
In trying to have it both ways Biden got nothing. Now a wider war is inevitable. Blinken's policy is in shambles. The failure was from the top. We need a new strategy. The old one is dead.
— wretchardthecat (@wretchardthecat) April 14, 2024
Here's Styx's more neutral commentary. I disagree with most of what he says here.
Scott vs. the bear
If you're upset by the sight of Ballistic Dummy Labs skulls, torsos, etc. being shot to pieces, then please don't watch this. In this video, Scott shows what happens to a bear's skull when it meets the titanic force of a 4 Bore rifle round:
Monday, April 15, 2024
10,000K, 50 km per day, with a 50-kilo backpack???
Headline (via ROK Drop):
CHINESE WOMAN ON 10,000 KILOMETER HIKE LOOKS LIKE SHE HAS AGED BY 30 YEARS
A Chinese woman in her 20s who went on a 10,000km long hike turned into a grandmother in her 60s in three months.
According to the Hong Kong South China Morning Post on the 10th, Xasha (28), from Hubei Province in central China, departed from Chongqing City in southwest China in January and embarked on a walking tour to the Tibetan Autonomous Region. With a backpack weighing 50 kilograms, the walking distance so far is about 10,000 kilometers.
Sasha, who walks about 50km a day, receives donations through live streaming online from time to time. When there is a lot of donations, it is about 10,000 yuan (1.87 million won) per month.
A Chinese influencer filmed her hike and posted it on social media. What made headlines was her face, not her hiking scene.
This is because she did not wear makeup and her sunburnt face looked different from her previous appearance. On social media, “Your face looks 58 years old (not 28 years old).”
I don't think I could hack that, especially not in my current debased state. I did, however, leave a comment over at ROK Drop:
A wide-brimmed hat (possibly with the back cut off to make room for the too-heavy backpack) might’ve been useful. She should’ve talked to me. Meantime, it’s too bad people are remarking on her looks instead of encouraging her. A 50-kilo pack sounds like overpacking to me, but it’s an impressive weight to carry for 50 km a day (which is also a super-impressive daily distance).
A 50-kilo backpack is insane: it's a soldier's load, and 50K a day is a soldier's distance. Maybe it makes sense if she's hiking through plenty of empty spaces, but otherwise, I'd say she should plan her walk better and have supplies either in caches or ready to be delivered to various waypoints. There are experts who hike the Pacific Crest Trail with only ten pounds on their backs—including water. Either something is off about the information in this article or the girl is just cuckoo. Anyway, good luck to her.
ADDENDUM: the math is funny. They say she started in January, and the verb tenses between the main article and the headline don't make it clear whether she's done. If she's done, then it's taken her roughly 105 days—assuming no rest—to walk 10,000 km. That's about 95 km per day, almost twice what the article claims. So I assume she isn't actually done yet. And how is she not dealing with blisters and other foot problems, given her load?
Something really doesn't make sense.
Dr. Ekberg hits me right where I live
This can only be viewed on YouTube. Note what Dr. Ekberg says about the relationship between intermittent fasting and treatments like exogenous insulin and metformin (which he views as fairly benign, but see Dr. Jason Fung below). Watch at 2X speed if you want. Meanwhile, here's one of the most important passages from Dr. Jason Fung's book The Diabetes Code:
Your doctor may prescribe a medication such as insulin injections, or perhaps a drug called metformin, to lower blood glucose, but these drugs do not rid the body of excess glucose. Instead, they simply continue to take the glucose out of the blood and ram it back into the body. It then gets shipped out to other organs, such as the kidneys, the nerves, the eyes, and the heart, where it can eventually create other problems. The underlying problem, of course, is unchanged. Remember the bowl that was overflowing with sugar? It still is. Insulin has simply moved the glucose from the blood, where you could see it, into the body, where you cannot. So the very next time you eat, sugar spills out into the blood again and you inject insulin to cram it into your body. Whether you think of it as an overstuffed suitcase or an overflowing bowl, it’s the same phenomenon all over again. The more glucose you force your body to accept, the more insulin your body needs to overcome the resistance to it. But this insulin only creates more resistance as the cells become more and more distended. Once you’ve exceeded what your body can produce naturally, medications can take over. At first, you need only a single medication, but eventually it becomes two and then three, and the doses become larger. And here’s the thing: if you are taking more and more medications to keep your blood glucose at the same level, your diabetes is actually getting worse.
Conventional diabetes treatments: How to make the problems worse
The blood glucose got better with insulin, but the diabetes got worse. The medications only hid the blood glucose by cramming it into the already engorged cells. The diabetes looks better but actually it is worse. Doctors may congratulate themselves on the illusion of a job well done, even as patients get sicker. No amount of medication prevents the heart attacks, congestive heart failure, strokes, kidney failure, amputations, and blindness that result when diabetes is getting worse. “Oh well,” the doctor says, “it’s a chronic, progressive disease.” Here’s an analogy. Consider that hiding garbage under your bed instead of discarding it allows you to pretend that your house is clean. When there’s no more room under the bed, you can throw the garbage into the closet. In fact, you can hide it anywhere you can’t see it: in the basement, in the attic, even in the bathroom. But if you keep hiding your garbage, eventually it’s going to begin to smell really, really bad because it’s starting to rot. Instead of hiding it, you need to throw it out. If the solution to your overflowing suitcase and your overflowing house seems obvious, the solution to too much glucose, which leads to too much insulin, should also seem self-evident: Get rid of it! But the standard treatment for type 2 diabetes follows the same flawed logic of hiding the glucose instead of eliminating it. If we understand that too much glucose in the blood is toxic, why can’t we understand that too much glucose in the body is also toxic?
[ ... ]
Standard medications do not prevent the progression of organ failure because they do not help excrete the toxic sugar load. No [fewer] than seven multinational, multicenter, randomized, placebo-controlled trials have proved that standard medications that lower blood glucose do not reduce heart disease, the major killer of diabetic patients. We have pretended that these glucose-lowering medications make people healthier, but it’s been a lie. We have overlooked a singular truth: you can’t use drugs to cure a dietary disease.
FACT: TYPE 2 DIABETES IS REVERSIBLE AND PREVENTABLE WITHOUT MEDICATIONS
Once we understand that type 2 diabetes is simply too much sugar in the body, the solution becomes obvious. Get rid of the sugar. Don’t hide it away. Get rid of it. There are really only two ways to accomplish this.
1. Put less sugar in.
2. Burn off remaining sugar.
That’s it. That’s all we need to do. The best part? It’s all natural and completely free. No drugs. No surgery. No cost.
The literature I got from the hospital before leaving says none of this—which is why I'm on metformin and insulin—and it's one of the reasons why I've said that I think Korean medicine is maybe 20 years behind (parts of) the West, and by extension one of the reasons why I still have trust issues about Korean medicine. One of the many books I'd been given at Samsung Hospital talks about the diet I should follow—a diet full of carbs (a little below the USDA 45-60% daily allowance). Jason Fung, meanwhile, stands at the cutting edge of diabetes research, but I can imagine how resistant Korean doctors would be to his advice. Here, timid conservatism trumps aggressive innovation. To be sure, if I read Fung's book and failed to follow his advice, that's on me, but it doesn't invalidate Fung's insights one bit.
I'm not following Fung's recommended diet right now, but I'm mindful of it. I'm back on Roy Taylor's Newcastle diet (from his Your Simple Guide to Reversing Type 2 Diabetes, suggested by my friend Neil) and will remain there for the next ten weeks. After that, I have to get strict about following keto, carnivore, or something extremely low carb.
One lingering issue to discuss is whether I'm in any position to question the experts given my dire situation. I'd say yes, at the risk of sounding stubborn. I'm not making judgments willy-nilly; I'm arming myself with knowledge from better experts and doing my best to make intelligent decisions about my own care. If I mess up in that care because of my own weakness of character, that's not a knock against the experts in the West that I've read, nor is it affirmation that the Korean docs have it right. And that's about where I stand on these topics.
a week of travail (3)
Friday turned out to be my last day; I'd at least heard that correctly. What I next needed to know was when I'd be getting my "education" so I could have an idea as to when I'd be leaving. Also: there's one important stat that I've forgotten to talk about this entire time: my pulse-ox. A pulse oximeter is a device that slips onto and shines a light through your fingertip, registering not only your blood flow but, more importantly, how oxygen-rich your blood is. It normally goes on an index finger, but I've had it on my middle finger, ring finger, etc.—whichever digit happens to be available at the time. Pulse-ox was definitely one of the numbers the staff was curious about; it's measured as a percent, with 97-100% being good to excellent. Start slipping down to the 92-95% range, and you're probably having a bit of difficulty breathing. I don't know what my pulse-ox was at home when I felt as if I were drowning, but at the hospital, I was around 92%. As long as I didn't exert myself, that range was fairly tolerable for me, but the moment I tried to walk any distance or lift something that would've been easy to lift had I been healthy, I'd feel the tight, invisible hand around my heart and lungs. By the end of my stay, my pulse-ox floated up from 92-ish to about 97-ish. Good enough to let me go, but they did put me on oxygen for a spell on Thursday.
At some point Thursday night, with my roommate having changed from the difficult old man to the introvert, I elected to blast my fan and take a shower. My hospital top had been changed because I'd been sweating so much, but my crotch and entire pants area was redolent with the stink of being unwashed for several days. I didn't shower, but I did the equivalent of having a sponge bath: I used the smart toilet's bidet function, along with some soap, to wash my nether regions. With no towel, I used toilet paper to dab myself mostly dry, then hand-washed my hair and my armpits. My torso was still covered with electronic sensors, so I couldn't do anything about that (by which I really mean that I didn't ask), but after washing my filthiest body parts, I felt some measure of renewal. Couldn't do anything about my underwear, alas.
Now, though, it was Friday morning. I had my breakfast at close to 8 a.m., and I heard that I'd be seeing a doctor (they used the Korean honorific term for professor to describe her—교수님/gyosunim) at around 10:30 a.m., and that I'd be let out soon after. Nice.
I texted my boss (he lives in Suwon, a satellite city south of Seoul) and told him not to bother coming; I'd be done early, and I'd see myself out. The order of events was: get the electronic readers taken off me, see the professor about my education (which I realized would be mostly about my new insulin pen), put my regular clothes back on, walk down the hall to pay my undoubtedly expensive bill, then get the hell outta there. 10:30 rolled around; my chest was free of those sensors although there was still some residual sticker gum leaving goopy traceries on my skin. I got into a wheelchair and was rolled to the elevators. Because I'd been lodged on the 16th floor, pretty much everything except ultrasound was beneath me (ultrasound was also on the 16th). We took the elevator down to 2 and rolled out. I was taken to the Diabetes Education Wing, and within a few minutes, I was greeted by a middle-aged, female doctor who, like almost all of the other docs, immediately asked me whether I could speak Korean.* My noncommittal "A little" allows them to permit themselves the luxury of speaking in full-speed Korean; I catch a healthy percentage of what they say and can guess a lot via visual cues (pointing, gestures, things they write for my benefit), and thus the lecture began.
It was indeed mostly about the insulin pens that would be a part of my life over the next few months. (I don't really need them, just as I don't need the drug metformin despite a prescription for it; you'll see a post on this point later this evening that argues that insulin and metformin only make my problem worse.) But we did go over things like diet (they have ridiculously lax carb standards). I had the chance to practice using the insulin pen on a sort of rubber ball held inside a mount to keep it from rolling; the ball simulated flesh. It took me three practice runs before the doc was satisfied, and she gave me a set of books and pamphlets on diabetes for my edification as I left. I did manage to ask some questions before going, though, and I learned that (1) my problem was definitely not related to COVID,** (2) the insulin shots—which I'd made clear I hated—wouldn't be a permanent thing, but a lot of that was up to me, and (3) repair of my heart would be a matter of following the meds schedule, dieting strictly, and exercising more and more. This did leave me a bit confused, though, because I would've thought the road to recovery for someone supposedly on the brink of death would be a lot less blasé and a lot more specific and strict. Such does not seem to be the case: take zee pills, do zee injections, diet, and exercise without over-straining. No one said I had to worry about being a ticking time bomb who would collapse at any time—no one but that self-righteous doctor at the beginning. So I feel as if I'm in about the same place as I was three years previous. I know that the Newcastle diet had me losing a ton of weight over three months (about 28 kg or 62 pounds), my HbA1c score went down to 5.7 (practically non-diabetic), and my aggressive walking had helped my heart and lungs. Add stairs to that, diet more strictly this time, and that's a winning formula. With many thoughts swimming in my head, I was rolled back to the 16th floor.
Once back on 16, I eagerly changed into the clothes I'd been admitted in the previous Monday evening; a nurse explained the bill-paying and meds-receiving procedure; it all seemed simple enough. My final bill was W1,427,470, less than half my bill from three years ago. I'd stayed at the hospital for less time, and I'd had fewer tests done on me. They had my citizen's ID number, which in theory is linked to my national insurance policy, so I assume insurance played a role in the calculation of price. The place to pay was also on the 16th floor (I wonder whether there's a cashier on every residential floor; they certainly want your money). I was handed some final paperwork that included the dates for my next appearances at the hospital: at the end of this month and on May 24.
Final self-assessment: my pulse was still a bit high, as was my blood sugar, but my blood pressure had been brought under control, and my pulse-ox was near optimal. I had also lost a few kilos. I was still weak and not able to walk long distance, and hefting my Costco bag full of things (it was the boss's Costco bag) was a bit of a chore. Since I'd been given a few weeks' worth of meds, there was no need for me to visit a pharmacy, but I did need to visit a medical-supply store to pick up a constant glucose monitor (in the US, and apparently also in South Korea, there's no longer a need for a prescription to buy this machine). I still haven't done that, but I will do so tomorrow (Tuesday) morning. The CGM tracks your blood-sugar levels all day long; you fasten it onto your shoulder right at the deltoid; it has tiny needles that barely pierce the skin. The moment you eat something, your blood sugar rises, and your body spikes insulin to bring the sugar back down. Insulin isn't the healthiest hormone: it reduces your blood-sugar levels, but it also primes your body to store fat. The object of the game, according to every expert I watch, is to minimize insulin spikes. This is why intermittent fasting and regular fasting are key; if you eat nothing, you have no spikes to worry about.
Having paid up and with no immediate obligations, I took the elevator down and walked out the main entrance, walked across the access roads to the taxi stand, and got myself a cab back to my place, about a kilometer down the street. It would be nice to think that all of this was over, but you and I both know it's not: the hospital will be back to monitoring me, and I'll have to watch for my frequent lapses of will and my post hoc rationalizations, not to mention my diet and exercise regimes. I got healthy once before, though, so I know I can do it again. The question is how to keep the benefits once I earn them.
Welcome to the rest of my life.
__________
*There was one flummoxed female doc who came up to me and gave a speech about something or other in competent but somewhat broken English. When she left, one of the nurses who had witnessed the information dump smiled from behind her mask and chirped, "She didn't know you spoke Korean!" I told the nurse I was, if anything, relieved to get that information in English. Medical Korean is still mostly beyond me. I learn terms as the need arises, but I'm always behind.
**I was left to wonder, though, how I could have been strong enough, pre-COVID, to do 1.25 staircases, then suddenly left weak with heart failure. Maybe I'll ask the next time I'm at the hospital in a couple of weeks.
 |
| It was a relief to walk up to my apartment's side entrance. |
 |
| Spring is here. |
 |
| insulin pens |
 |
| tiny black dots = pinpricks from blood-sugar sampling |
sex work isn't "just work"
If you see no moral difference between working in a cubicle all day long and giving blowjobs all day long, then you're morally obtuse:
a week of travail (2)
Tuesday-Thursday, April 9-11, 2024
Monday night saw me moved from the emergency room to a berth on the 16th floor, in the cardiac ward. A lot about this felt familiar, and over the next few days, I ended up going through many of the same routines I had gone through when I'd had my stroke: for example, frequent checks of my blood pressure and blood-sugar levels all through the night. I had one CT scan on Tuesday (a computer voice commanded me to take breaths and hold them, then release) and several x-rays, plus a couple more thoracic ultrasounds. There was no MRI, perhaps because I'd said that lying flat on my back was causing me breathing problems, and an MRI would involve lying flat and still for thirty minutes—something I wasn't able to do. Or, for all I know, there was no MRI because one wasn't needed. I was only rarely subjected to cognitive tests like "What's your name?" and "What's your date of birth?" Mostly, whenever the nurses came by to do procedures, they would simply scan my wristband, which had my info and a bar code on it. Before I moved to the cardiac ward, I was given a set of hospital clothes to change into—the You Are Officially Sick and Belong to Us moment. I had no idea, at the time, how long I'd be remaining at the hospital. I assumed the staff's goal was to stabilize my heart and lungs, then educate me on what I'd be doing once I was out of the hospital.
I was also back on hospital meals, but I was given no choice as to whether I'd be eating from a Korean or a Western menu: the staff simply put me on the Western food, a fact that I took passively, not bothering to request a change to a Korean diet. I recalled that, three years earlier, the Korean menu billed as "for diabetics" included a lot of rice, a carby and seeming unwise choice for someone coming in with high blood sugar. The Western menu turned out to be just as nonsensical: for my first breakfast Tuesday morning, I got a weird combination of leafy-green salad and cereal. It was hard for me to work up an appetite; everything made me feel vaguely nauseous—not because the food was bad, but simply because. The only things I really enjoyed from the breakfast tray were (1) the coffee, which came with Equal sugarless sweetener; (2) a tiny carton of milk; (3) a tiny cup—barely a swallow—of orange juice; and (4) some slices of pre-peeled orange, all ready to be gulped down. There were hard-boiled eggs as well, and I had one but couldn't eat the other. I might have eaten some of the cereal (unsweetened cornflakes); I don't recall finishing it. Along with that first breakfast came a sheet with a list of lunch items; from then on, I could check which food items I'd like. Presumably, everything on the list had been pre-approved, including the carby dinner rolls. Over the next few days, my meals went that way: I'd get my meal plus a check-off list for the following meal. This got me into a prisoner's mentality: after a rough start with no appetite, I started looking forward to mealtimes as the highlight of my otherwise dreary days.
My boss, being my bohoja/guardian again, visited me periodically. He dutifully went to my apartment to pick up items I'd need to survive the heat and discomfort of hospital existence: my stupid-looking, thick-framed glasses (so I wouldn't have to constantly put on and take off my contacts); my mini electric fan so I wouldn't be sweating up a storm; my cell-phone charger. He even brought me an extra pair of socks; Koreans have a thing about holey socks, but I didn't put those new socks on until my final day.
I was moved, late Tuesday if I remember correctly, to another berth because my boss couldn't be with me 24 hours a day. This was a special berth that was staffed with more people who could watch over me in place of the bohoja. Otherwise, the routine tests continued, including a new one to me: a weigh-in. I'd started off at 118 kg, still 10 kg below my worst-ever weight, and by the time I left the hospital, I was down to 113 kg.
Another thing they had me do was log my urination history. They forced me to piss more frequently by pumping me full of diuretics (chemicals that help expel urine from the body); I got to a point where I was pissing an average of 500 cc every 45 minutes, and on Tuesday, I astounded myself by excreting over two liters of urine. How the hell had I contained that much? I joked to my boss that, one day, they'd cut open my cadaver, look at my internal organs, and marvel at the sheer size of my bladder.
I think I had three roommates in all. One was an old man who couldn't sleep while my fan was on, so I had little choice but to shut the fan off and suffer through the night, sweating. He later apologized for having been difficult, but I waved his apology off while secretly cursing him. The nurses gave me a "cold pillow" during that night to alleviate my suffering; I guessed that they kept the ward's temperature at around 26 or 27ºC, which is great for women, who generally like a warmer office environment, but hell on us guys. My preferred office temp is around 22 or 23 degrees. When the old man left Wednesday afternoon, he was replaced by a very quiet man who was in for cardiac surgery. I never found out what kind, but I've heard that stent installation is a fairly simple procedure; he seemed to be in and out of surgery fairly quickly. His wife proved more talkative than he was; he struck me as even more introverted than I am while the Missus proved a lot more talkative. I didn't get a good look at him until my final day, which is when I realized he was fairly young-looking. The old man and the introvert were my two final roommates; I can't remember who my first roommate was.
Wednesday was a parliamentary election day in South Korea, and my boss and his family had things to do that day, so I had no visitors. On Thursday, my Korean coworker took the bohoja pass from my boss and visited me. I had also heard from the doctors and nurses around me that I was supposed to meet a team at around 1:30 p.m. to get educated about what to do post-discharge. But at around 1 p.m., my blood pressure dropped precipitously; I was woozy and ready to faint, but I fought my way to the bathroom, had another piss, logged the volume of urine (around 400-500 cc), told the nurses how I was feeling, and got treated. By the time my BP had stabilized, there was no way I could make the Thursday-afternoon meeting, so it was rescheduled for the next day. I could've sworn they'd said it'd be in the late afternoon, at around 3:30 p.m., but I guess I misunderstood. (The meeting also turned out to be with a single doctor, not with a team. I really have to improve my Korean.) Anyway, the BP thing was scary; I've never fainted before, and that's only the second time in my life that I've come close to doing so. I did somehow retain enough consciousness to snap a pic of the BP monitor showing a reading of 66/46—the lowest blood pressure I've had in my life, especially after years of being around 180/95 (which is also scary when you think about it).
To occupy myself, and since I couldn't rely on the hospital's WiFi to watch YouTube on my phone, I spent my time reading Lee Child's Persuader, a Jack Reacher adventure novel that will be the template for Season 3. Persuader ended up being the best of the Reacher novels I've read thus far, so I'm hoping Season 3 of the Amazon show does it justice.
Thursday ended like the other days—with more testing and BP/sugar checks, more weighings, and the occasional question about whether I was sneaking any snacks: the staff had gotten my BP down and stabilized (I was a classic 120/80 at one point), but despite their best efforts, my blood-sugar numbers were still very high, so they were left to wonder why the number was so stubborn. I don't blame anyone but myself for that although I still marvel that there are people who doubtless have worse numbers yet somehow avoid being in the hospital.
I'd also heard that Friday would be my last day in the hospital, but I wondered what time of day I'd actually be leaving if I had that afternoon meeting to look forward to.
Stay tuned for the conclusion.
 |
| the lowest BP I ever did see |
 |
| My Korean coworker dropped in late Thursday afternoon. |
Nick Freitas interviews Gary Buechler (Nerdrotic)
A long interview, but worth your while. Watch at 2X speed and be done in half the time:
Sunday, April 14, 2024
silat looks to be an interesting martial art
The key to mastering this style of combat seems to be getting inside the opponent's guard:
Part 2 is coming
It's been a lazy weekend of just resting since I got back from the hospital. I'm currently very weak, just like three years ago when I got out after my stroke. I imagine the weakness will last a few days. I'm normally sluggish in my movements, but I'm more sluggish than usual, and most of my muscular weakness feels as if it's in my shoulders: raising my arms above my head is a chore, and carrying anything heavier than empty cardboard boxes feels like a herculean effort. In the meantime, I've barely been able to summon the energy to stand, let alone write an extensive blog post. Expect something tomorrow, but today, Sunday, has been a day of rest. There are some scheduled posts on the way, but the main chronicle won't continue until tomorrow. Sorry and thanks for your patience. I have other posts on the way, too, and they might make an appearance later this week.
Meantime, what can I say? I can say that my breathing problem has mostly cleared up thanks to the care I received at the hospital, but I still have a bit of a stuffy/runny nose. The above-mentioned muscular weakness is frustrating, but I have faith that, as my body finds a new rhythm, things will even out, and I'll regain my energy. I want to get back into the exercise program that I had barely embarked upon before all this nonsense happened: dumbbells, calisthenics, kettlebells, heavy clubs, elastic bands, and animal flow—a little of each thing. I plan to restart the walking sometime this week, probably with some ridiculously modest distance, just to get back into the rhythm. By the end of April, I ought to be walking regular distances. In May, assuming my heart allows it, I'll start back with staircase work, maybe just up to the 6th floor, maybe farther. We'll see what the gods allow.
Just know that I haven't forgotten my duties. Expect more tomorrow.










what's different this time around?
It feels as if some things have changed at the hospital since 2021. Here an incomplete listicle of perceived alterations:
- PA announcements are more frequent.
- No more COVID testing protocols. I wasn't tested for COVID at all, and neither was my boss, who again acted as my guardian/보호자/bohoja.
- Wheelchairs seemed more solid, so wheelchair rides weren't as fun as they were before.
- X-ray tech seems to have radically improved. Maybe I'm mistaken, but getting x-rays used to be a bit of an affair. Now, they stand you up against a special background, tell you to breathe in so as to expand your chest, then to hold your breath, and just like that, you're done in 5 seconds.
- My roommates didn't fart as much, and when they did, they weren't nearly as loud and proud.
- Western meals. I opted for Korean last time, but this time, they simply put me on a Western-meal schedule.
That's all I can think of for now.

Saturday, April 13, 2024










pics from Wednesday
 |
| the miracle of berth |
 |
| sign warning about weak WiFi |
 |
| "cold pillow," all warm and melted now |
 |
| the fan currently saving my life |
 |
| living a life of danger |
 |
| the view out my current window |
 |
| hallway at night |
 |
| the outside of my berth |
a week of travail (1)
Here at last is Part 1 of the chronicle of my latest health misadventure. I have, frankly, little motivation to write this, but since I committed long ago to making certain aspects of my life an open book on this blog, I'm going through with the telling all the same.
Sunday, April 7, 2024 and Monday, April 8, 2024
Sunday night, I Skyped with my buddy Mike, who's based in Fredericksburg, Virginia. Everything seemed to be positive, but little did I know that, barely an hour after I finished talking with my friend, I would start having more breathing difficulties. These were bad; they kept me up all night, which made them somewhat scary: I got to a point where I began to wonder whether I'd live through the night, and by morning, that feeling that changed very little. I could feel my body's energy running out of me like sand out of the top of an hourglass, and a dim sense of urgency started to well up: Should I really go to the hospital? I hadn't wanted to go, and like a lot of people, I hadn't wanted to face the truth of whatever was going on. And what was going on? The more practical side of my brain reasonably noted that it's better to know than not to know (my boss echoed this thought a few days later), so at some point in the afternoon, after a whole morning of sitting against the wall, staring at the ceiling, vainly trying to breathe, and feeling as if I were beginning to drown, something clicked, and I decided I wanted to live, even at the expense of potential humiliation. Gathering my strength up to do the next thing felt as if it took years, but even if it wasn't years, it was hours. I somehow heaved myself up, got dressed, left my building, and caught a cab to the building where I worked because it also has a clinic where I visit my regular doctor.
The doc ribbed me for not visiting before now; I had run out of stroke/diabetes meds last year, but I hadn't come back for my checkup and refill in months. I lied that I'd been busy; I'm sure he saw through that. From an introvert's perspective, one of the nicer aspects of doctor visits in Korea is that the doc isn't interested in keeping you long. Most such visits don't last longer than 5-10 minutes if you're there for a consultation, and they rarely go beyond thirty minutes if you discover you're there to be tested. Monday's visit involved several tests, but even with those, my time with the doctor didn't last much longer than, oh, 40 minutes. There were the usual tests: blood sample (normally done once every 3-4 months), urine sample (usually to check glucose levels among other things), and a check of my pulse and blood pressure. BP is always high for me, partly because it's always naturally high, and partly because, on some level, clinics and hospitals stress me out. When I told the doctor about my breathing issues and thready pulse, I exercised my just-learned vocabulary and floated the idea that I was looking at myocarditis (shimgeunyeom/심근염, heart-sinew [in]flame[ation], inflammation of the heart muscle). The chronology made this make sense: I'd re-contracted COVID back in mid-March, and myocarditis can rear its head—sooner or later—after an infection although, from what I'd seen, it seemed more likely in people who'd gotten jabbed. Some sources listed myocarditis as "rare," jabbed or unjabbed, but this didn't make me feel special.
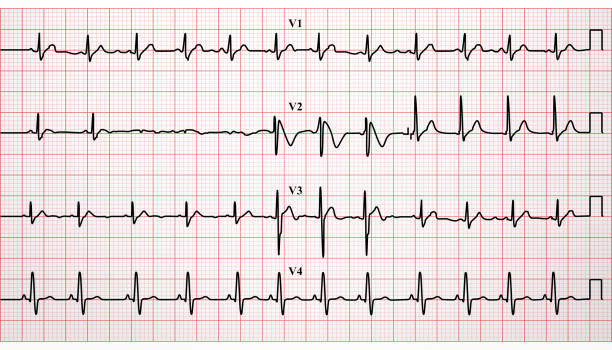
After this further explanation of my current symptoms, the doc ran two more tests: an EKG (or ECG, i.e., an electrocardiogram, which shows several parallel graphs of your heart's performance) and a chest x-ray. We didn't focus on the x-ray, but the doc didn't look happy when he saw the EKG. He looked, in fact, as if he couldn't make heads or tails of what he was seeing, and he advised me to visit a hospital that had better facilities to get some further testing and treatment. This is the moment that set me on the path to another hospital adventure, and I wasn't feeling hardy enough to walk out of the clinic and simply ignore his advice. What I did do, after I'd been issued a prescription, was to walk back downstairs (the clinic was on the second floor), walk across the building, then walk up the stairs to my company's office, where I saw my boss and coworker. They hadn't been expecting me because I'd texted them earlier in the day about feeling under the weather. When I explained the situation to my boss and told him I wanted to pick up my prescribed meds since the pharmacy was along the way to the hospital (these were specialized meds not available at every pharmacy; there's one specific pharmacy that I have to go to), he offered to give me a ride to the pharmacy and then to Samsung hospital. (I'm reverting to the standard "Samsung" spelling instead of the more governmentally accurate "Samseong.")
As I suspected would happen, the pharmacy, called Blue Bird Pharmacy (파랑새 약국, Parang Sae Yakguk), wasn't able to provide me my meds. This happens every time I go there: there's usually one or two meds that aren't in stock, so the staff comes up to me apologetically and says it has to order the missing meds, and that I should come back a day or so later to get everything. I cynically mentioned this to the pharmacy staff in anticipation, but they said, "Oh, no—this time, the problem is different: the way the prescription had been written was wrong." Although the prescription needed to be filled within 3 days, the time period for the prescription didn't start until June, which made things awkward for the pharmacy (Koreans obey or ignore rules in a seemingly random way: why not cut me a little slack, this time, instead of suddenly being all by-the-book?). I vaguely recalled my doc saying something about timing, but I hadn't understood him that well. Maybe he'd been trying to say that, before I went back to my regular stroke/diabetes meds, I needed to get checked out and prescribed other medicine first, then I could restart my regular meds in June. I'm just guessing, of course: I have no idea what he actually said or meant. All I knew was that the 'scrip had been a waste of time and effort. Anyway, the end result was the same: the pharmacy let me go back to my boss's car empty-handed, and we sped on up to the hospital, which was just up the street. Had I been healthy, I could've walked from my apartment to the hospital.
Once you enter Samsung Hospital's main entrance, you follow a labyrinthine series of access roads to reach the emergency room. My Korean coworker had elected to come along with us, and he pointed out that the hospital would end up prescribing equivalent meds, anyway, so the failed errand at Blue Bird Pharmacy wasn't tragic. We pulled up to the ER entrance; I got out with my coworker while my boss went to find a place to park. My coworker and I were let in by a guard/staffer, and since I was already in the system as a patient from three years previous, there was much less paperwork to fill out. I waited with my coworker to be called into some sort of intake-interview room; the procedure felt a bit different this time. The wait was long enough that my boss was able to rejoin us after parking. When a young, male doc or staffer finally called me over to the interview room, the ensuing conversation took place in a mixture of Korean and English. I was glad the boss was there; his Korean is fluent whereas mine is inadequate for discussing technical medical problems. A short history of my problem was taken, then I was taken into the ER itself. My coworker couldn't follow us there; my boss had once again been designated as the bohoja/보호자, or guardian, so only he could accompany me into the guts of the hospital. My coworker, looking tired, went home.
I was given a thoracic ultrasound and some drugs to help stabilize the breathing; hours passed. A somber, self-righteous-sounding doctor came up to my berth hours later with the news that my problem wasn't related to COVID at all: I was looking at a species of heart failure. This absolutely floored me, but I made an effort to keep a poker face. I had expected to hear the usual finger-wagging about needing to eat better and exercise, but as my boss interpreted the parts I didn't understand, I was left with the impression that they were saying my condition had been caught just in time, and that a lack of treatment would probably mean my death. Most people have heard of congestive heart failure, but my condition was, specifically, "severe left-ventricular systolic dysfunction." (Read more here.) This was well beyond a merely weak heart: this was close to the actual death of a large part of my cardiac muscle. The doctor said, in that finger-wagging voice of hers, that this was partly a result of my fateful choice, three years ago, not to stay at the hospital for further treatment. This decision didn't seem at all irrational to me at the time. Still doesn't.
So, near as I could figure, the chronology of my condition went back way further than my recent mid-March bout with COVID. This is something that had compounded over time. The other revelation was that this was fundamentally a heart condition, not a lung condition, even if the breathing issues felt, subjectively, as if they were the most urgent problem. The causal chain was: heart problem first, breathing problems next. Fix the heart, fix the breathing. My boss said the doctor was basically saying that, if nothing were done about my condition, I'd die. So: what would fixing my heart entail?
The irony of my life is that one of the things I fear most is being a bother to others. I consider myself a fairly independent person. It's the thing I stress when I rant about expats who never bother to learn the local language beyond a few pidgin phrases: such people, through their own laziness, consign themselves to becoming linguistic cripples who have to depend on everyone around them in order to navigate daily life. A Western guy comes to Korea, quickly acquires a Korean girlfriend, then uses her like a slave to help him out with daily tasks like navigating the bank, dealing with the tax office, or dealing with everyday issues and problems that require more than a 101-level knowledge of the local language. Maybe the girl is okay with this situation and sees this as her lot; if I were in the guy's place, I'd feel like a bother, so I've made sure that I can do all of the aforementioned tasks on my own. What's ironic is that, thanks to my choices and habits, I was now in the hospital again, basically being a bother to everyone. And lacking the language to handle more than the basics of my situation.
At the same time, I couldn't help feeling a sense of cosmic injustice about my circumstances. They say that well over 50% of Americans are obese, and 30% are morbidly obese. There are plenty of Americans who are wider than they are tall, and as bad as my own eating habits might be, these people are undoubtedly worse... and yet, they never seemed to end up in hospital. (This is a subjective impression, mind you; I don't know the real facts.) Also: how did I go from 1.25 staircases from January through mid-March to being laid up in a hospital bed in April? Were my own habits that bad? Could it just be a matter of bad wiring, like the people who joke that they just look at a piece of chocolate cake and gain ten pounds? Dr. Sten Ekberg, in his YouTube videos on diet and exercise, has said that there is, in fact, a strong genetic component to health. There are people with dynamo metabolisms who burn up anything they put into their bodies; there are other people, like me, who are cursed with sluggish metabolisms, thus requiring us to work harder to be healthy. That's life, and a lot of success is about figuring out your own level and playing the cards you've been dealt. I tentatively conclude that, along with my own dietary misconduct, I've been dealt a bad genetic hand. My mother's father died of a heart attack; my maternal grandmother was born with a strange genetic condition: an upside-down stomach that prevented her from digesting anything properly. She never got above 70 pounds, according to Mom. My paternal grandparents were alcoholics, and I think they both died of alcoholism-related heart attacks. My own dad, a teetotaler, had a heart attack in 2006. So my family tree points like a dagger right at my heart. I vaguely recall that, when I'd had my stroke in 2021, I mentally chuckled about dodging a karmic bullet. But, it seems, the cardiac monster has been after me this entire time.
So I grudgingly chose to be admitted. My boss, seeing my face and hearing my tone, joked with the self-righteous doc that I was stubborn. He had a wife and family to go back to, so he couldn't stay, and I was left with the realization that, like Jimmy Stewart in It's a Wonderful Life, what happens to me affects others, pulling them away from their own lives so as to deal with my lame, dependent ass. I personally have little to no fear of actual death; while my life has its discontents, its wishful pangs related to counterfactuals—the would-haves, could-haves, and should-haves—I'm generally content with how things have turned out, and if it's time for me finally to spill over the edge of the conveyor belt, I'm fine with that. But like it or not, I'm going to end up being a bother to somebody because, as I've long known from reading about Buddhism, we're all connected in some way, like it or not.
And that's how I ended up in the cardiac ward, 16th floor. Let the poking and prodding begin!
To be continued.










reactions to my situation
Here's what I wrote in an Instapundit open thread:
After training on the staircase for two-and-a-half months, I got COVID again around mid-March (I remain resolutely unjabbed). All my routines went out the window. Luckily, I didn't lose my smell and taste like last time. But I did have trouble with my breathing and heart rate, so I wondered if this was myocarditis. Finally went to my local doc; he did some tests, including x-ray and EKG, then he said, "Get thee to a local hospital for more detailed testing. I don't like what I see." So I went to the same hospital that treated me when I had my stroke three years ago, and they said, "Nope, it's not COVID-related myocarditis. It's heart failure—severe left-ventricular systolic dysfunction." So I'm left to wonder how that's possible. Once a year, I walk across Korea, which means plenty of practice walks throughout the year. I realize my eating habits aren't the best, but enough to contribute to heart failure?? Anyway, they say therapy is possible; the hospital is drugging me up and monitoring me for the moment, then they'll tell me how I need to lead my life from now on, I guess. I'm still pondering how I went from walking 1.25 times up my apartment's staircase (B1 to 26, then B1 to 6) to lying in a hospital bed. Frustrating. Default assumption is that I did this to myself, and it all comes down to diet, but if this smart group of people* has other ideas, I'm all ears.
Responses came in within a couple hours:
1. As I recall, you are a fairly young guy too, especially for this place...any family history? Maybe get a second opinion too? Sorry I can't offer more...I've always admired your walking trips and the training you described...good luck with everything...
2. I don't know if it is one of Murphy's Laws, but it is a law nonetheless: you can be doing everything you should be doing in the way you should be doing it, and not be doing what you shouldn't do, and still end up "behind the eight ball."
So there I was in ICU, the doctor came in, introduced himself, and said: Mr. Sam, you're a mystery. You have X, Y, and Z, and no risk factors.
3. Eh, sometimes health problems just happen, despite one's best efforts.
If it makes you feel better, your fitness regimen is likely to give you a better chance of recovering faster, if they can fix your heart.
The important part is, they found the problem before you dropped dead of it.
4. It's not something you did; it's the human condition. I hope you deal with it successfully.
5. I had a former coworker who was the most health-conscious, right-eating, exercise-maniac person I ever met. He went into the doctor after three or four months of just not feeling right, having difficulty working out, all that jazz; the verdict was congestive heart failure. Sometimes it’s the luck of the draw and there’s nothing you can do about it.
6. A sub-optimal diet can absolutely contribute to heart failure. Doctors like to recommend low fat, low saturated fat, and low salt diets for heart patients. But you can solve 80% of your health problems by eating in a way that minimizes blood sugar spikes.
Context: My family is Chinese and has a history of both heart disease and diabetes. My mom is a Buddhist vegetarian and was baffled to find that she had high cholesterol and high blood pressure despite not eating any saturated animal fats. It was the sugar and processed carbs that caused the problems. My dad's dad was a baker by trade, and unsurprisingly type 2 diabetes is a problem on my dad's side of the family. But heart disease is also a problem on my dad's side because blood sugar issues can cause clogged arteries.
Books I like about the effect of high blood sugar levels on overall bodily health:
- Obesity Code by Jason Fung
- Glucose Revolution by Jesse (forgot last name, starts with an A)
- Why We Get Fat by Gary Taubes
I like this book written about cancer (even though I do not have cancer) for its message that we can take control of our own health rather than blindly following medical advice that may or may not be in our best interest:
- Radical Remission (forget author's name)
Best of luck to you in your health journey.
7. James (Jimmy) Fuller Fixx (April 23, 1932 – July 20, 1984) was an American who wrote the 1977 best-selling book The Complete Book of Running. He is credited with helping start America's fitness revolution by popularizing the sport of running and demonstrating the health benefits of regular jogging. He died of a heart attack while jogging at 52 years of age; his genetic predisposition for heart problems and other previous lifestyle factors may have caused his heart attack.[1]
I've lived in Korea long enough to be conditioned to expect a lot of blame-and-shame (commenter #6 is ethnically Asian; his response at least somewhat fits the pattern), so this unwillingness to blame me feels surprising and a little off (through no fault of the commenters), especially since conservatives preach the gospel of Take responsibility for yourself. I'm still waiting for one or two of the doctors on the board to weigh in; the average age of an Instapundit commenter is around 60, and many of these people Know Things. I'll post an update if there are any other responses.
__________
*I'm referring to the Instapundit commentariat.
Subscribe to:
Posts (Atom)




{kind=link}